
On January 17, 2017, industry think-tank the Fraser Institute released a new report, Did the Coal Phase-out Reduce Ontario Air Pollution? which suggests that coal plants across Canada should not be phased out based on its assertion that Ontario’s phase-out did not significantly reduce air pollution (Fraser Institute, 2017). This report includes a number of statements about pollution, health care benefits, and coal plants that are incorrect or misleading.
The Fraser report focuses on the air pollution benefits of the Ontario coal plant phase-out while ignoring the many co-benefits associated with this action. In 2002, the five coal-fired power plants in Ontario were responsible for
- nearly one quarter (23%) of the sulphur dioxide (SO2) emissions and one seventh (14%) of the nitrogen oxide (NOx) emissions in Ontario that contributed to air pollution and acid rain,
- nearly one quarter (23%) of the airborne mercury emissions which contributed to the contamination of fish with a persistent toxic that is harmful to the brains of humans, and
- one fifth (20%) of Ontario’s greenhouse gases emissions that were contributing to climate change (OPHA, 2002).
Over the last 20 years, the public health sector, the Ontario Medical Association, environmental organizations, cottagers’ associations, and labour organizations have been outspoken advocates for the phase-out of coal plants in Ontario. All of these groups shared the common view that many health and environmental benefits could be gained simultaneously by closing Ontario’s coal plants.
While there were technologies that could be applied to reduce emissions of sulphur dioxide, nitrogen oxides, and mercury from these plants, there was no technology at that time that could eliminate emissions of greenhouse gases. Given the age of Ontario’s coal plants, the availability of combined cycle natural gas plants, the promise of energy efficiency, and renewable technologies, it made more sense economically to accelerate the closure of coal plants than to re-invest in them.
The Fraser report and press release suggest that coal plants are not a major contributor of fine particulate matter (PM2.5)—the air pollutant that has been mostly clearly linked to chronic health impacts such as heart disease and lung cancer, and one of two air pollutants responsible for most of the smog alerts that used to be common in Ontario. This is simply not true.
Coal plants emit significant quantities of SO2 and substantial quantities of NOx. Both are gaseous air pollutants that can harm human health directly. When they enter the atmosphere, they can be transformed into sulphates and nitrates—acid particles that contribute to air levels of PM2.5. In fact, this secondary PM2.5 is the major culprit behind high levels of PM2.5 measured in many airsheds and is often more hazardous for human health than other forms of PM2.5 (RIAS, 2011). This PM2.5 does not, however, show up in emission inventories for PM2.5.
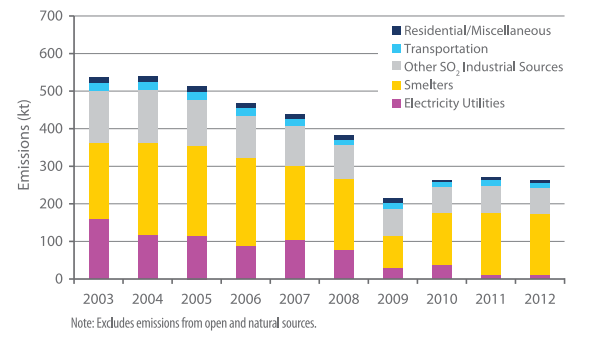
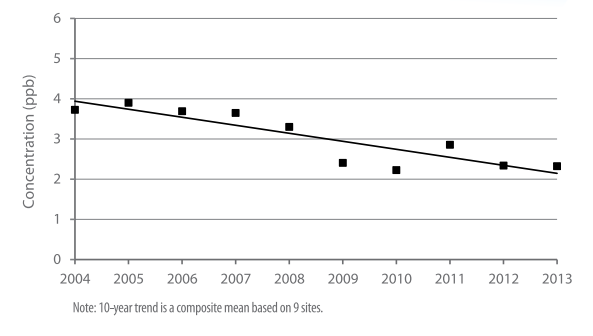
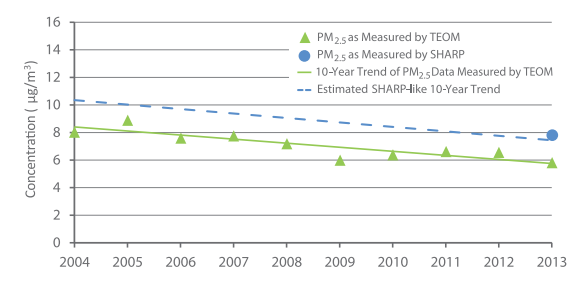
The Fraser Institute suggests that Ontario’s coal phase-out had little impact on emissions and air quality. This is misleading. Between 2003 and 2012, SO2 emissions from coal plants were reduced by about 140,000 tonnes (see Figure 1). During that same period, annual air levels of SO2 across Ontario declined by nearly 50% (see Figure 2) and annual air levels of PM2.5 declined by about 25% (see Figure 3) (OMOECC, 2014). While the improvements in air levels of SO2 and PM2.5 cannot be attributed solely to the closure of coal plants, their closure was an important contributor to reductions in air levels.
Air quality is impacted by multiple sources of pollution. The actions to reduce air pollution are intentionally broad-based because the improvements are cumulative. Coal plants are an efficient target for emission reductions because they are stationary sources that emit large volumes of air pollutants. They are also a significant source of air toxics such as mercury and greenhouse gases.
Air pollution is also a transboundary issue. Emissions of SO2 and NOx from coal plants in the U.S. have a significant impact on Ontario’s air quality, while emissions from Ontario’s coal plants have a substantial impact on air quality in Quebec, Vermont and New York (Yap et al., 2005). In recognition of this reality, Canada and the United States committed in 1991 to take action on both sides of the border with the Canada-US Air Quality Agreement. This agreement has proven very successful. Emissions and air quality on both sides of the border have improved because of cooperation between the two countries (Canada-US, 2014).
In 2005, Ontario estimated the contribution of coal plants to air pollution across Ontario and the adverse health impacts associated with that contribution. Because coal plants release air pollutants so high in the air, the pollutants are dispersed over long distances. The impact, therefore, on any one airshed is relatively small, but the impact overall on human health can be significant because so many people can be affected. Using methodologies that were well-accepted in other jurisdictions, Ontario estimated that air pollution from its coal plants were responsible for over 600 premature deaths, 900 hospital admissions, and 1000 emergency room visits, each year, in Ontario. These health impacts were valued at $3 billion per year (OMOE, 2005).
The Fraser report suggests that the $3 billion in health benefits estimated cannot be accurate because it represents too great a percentage of Ontario’s health care budget. This statement reflects a misunderstanding about the health benefits estimated in 2005. The $3 billion per year in health benefits reflect the value of the many lives that are shortened by air pollution, as well as health care costs. They do not reflect health care costs alone. The 2005 report is clear about this point.
An independent assessment conducted by Toronto Public Health in 2014 suggests that improvements in Ontario’s air quality have translated into significant health benefits for Ontario residents. Toronto Public Health found that improvements in Toronto’s air quality from 2000 to 2011 have reduced air pollution-related premature deaths by 23% (from 1,700 to 1,300 per year) and hospital admissions by 41% (from 6,000 to 3,550 per year) in Toronto alone. It attributes the improvements in air quality to a variety of policies implemented by different levels of government including the phase-out of coal plants by Ontario (TPH, 2014).
With the evidence of catastrophic climate change mounting daily, the need to modernize Canada’s electricity sector has never been more clear. With the costs of renewable technologies dropping, the opportunity to transform our economy has never been greater. CAPE stands by its position. We believe that the phase-out of coal plants in Alberta and across Canada is an economically prudent decision that will improve the health of Canadians while taking the steps needed to address climate change.
Prepared by Kim Perrotta, MHSc, Executive Director, CAPE
References:
- Canada-US, 2014. Canada-U.S. Air Quality Agreement Progress
- Fraser Institute. (2017). Did the Coal Phase-out Reduce Ontario Air Pollution? Prepared by Ross McKitrick and Elmira Aliakbari.
- Ontario Ministry of Energy (OMOE). 2005. Cost Benefit Analysis: Replacing Ontario’s Coal-Fired Electricity Generation. Prepared by DSS Management Consultants Inc. RWDI Air Inc. April, 2005
- Ontario Ministry of the Environment and Climate Change (OMOECC). 2014. Air Quality in Ontario 2013 Report.
- Ontario Public Health Association (OPHA). 2002. Beyond Coal: Power, Public Health and the Environment
- Regulatory Impact Assessment Study (RIAS). 2011. Reduction of Carbon Dioxide Emissions from Coal-Fired Generation of Electricity Regulations.
- Toronto Public Health (TPH). 2014. Path to Healthier Air: Toronto Air Pollution Burden of Illness Update. Technical Report.
- World Health Organization (WHO). 2013. Review of evidence on health aspects of air pollution – REVIHAAP Project.
- Yap, David, Neville Reid, Gary De Brou, and Robert Bloxam. 2005. Transboundary Air Pollution in Ontario 2005. Queen’s Printer.

